Chirally Pure S-Metoprolol - Place in Therapy
Dr. Arup Dasbiswas,Dr. Debasri Dasbiswas
Director – Institute of Cardiovascular Sciences and Head of the Department – Cardiology ICVS, IGPMER and SSKM Hospital, Kolkata
Associate Professor, Department of Pharmacology, N.R.S. Medical College, Kolkata.
INTRODUCTION
The term chirality is derived from the Greek word “kheir” meaning ‘hand’. An object is called “chiral” if it is not superimposable on its mirror image. “Chirality” refers to the spatial orientation of objects including molecules. Molecules must interact with receptors, enzymes and binding sites for their absorption, distribution, metabolism, excretion and action. This interaction is stereospecific and depends on how closely the three dimensional structure interacts or fits onto the three dimensional receptor or binding site. Thus similar looking mirror images may not conform stereo-specifically to such binding sites. Just as one would not wear a right shoe on the left foot or a right handed person would not try to write with the left hand, the orientation of molecules is vital for proper pharmacokinetics (what body does to the drug) and pharmacodynamics (what drug does to the body).
Most beta-blocker drugs possess one or more chiral centers (an asymmetrical center) that confers non-superimposability between the mirror images of the molecule. In fact, mixtures of enantiomers available as racemate drugs may be considered as fixed-dose combinations of two different molecules, and sometimes may pose as much irrationality as many fixed-dose combinations of different drugs we are aware of. The science of “chirality” includes the synthesis of single enantiomers, their intermediates and chiral “switches”. In a “chiral switch”, the more useful enantiomer is isolated from the mixture (racemate) and presented as an improved single enantiomer (unichiral) chemical entity.
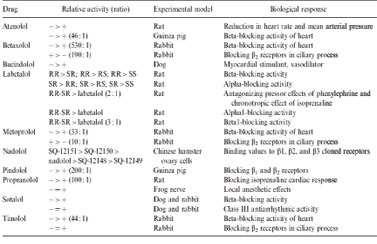
enantiomers in order to avoid potential harm to patients that might be derived from the non beta-blocking d-enantiomers the more so as the synthesis of the optically pure d- and l-enantiomers of any beta-blocking drug is easily feasible today, even on an industrial scale and at low costs, and that only half the dose of the optically pure l-enantiomers is needed to obtain the full effect of the currently used racemic mixtures.” It may be noted that d and l (abbreviated for of dextro and levo) describe the optical activity of S or R enantiomer; for most beta-blockers d is R and l is S. Table 1 illustrates many of the differences between beta-blocker enantiomers13.
Till recently, Timolol was the only beta-blocker that was marketed solely as the S-enantiomer for systemic administration. In India, S-Atenolol was introduced in 2003 followed by S-metoprolol succinate in 2005. In this review, we will discuss S-metoprolol in detail.
S-Metoprolol Succinate:
Correspondence: Dr. Arup Dasbiswas, Director , Head of the Department Cardiology ICVS, IGPMER and SSKM Hospital, Kolkata, West Bengal, Insia
Email:arup2415@dataone.in
|
The b1 receptor affinity of the S-form is about 500 times greater than that of R-form.2 An in-vitro animal study evaluated stereoisomeric pairs of Metoprolol for their ability to block b-2 receptors. This study showed that that the R-enantiomer was much more potent relative to the S-form, with activity ratio of 10 in blocking b2 receptors.3 While, a preferential metabolism of R-Metoprolol in extensive metabolizes (EM) results in a S:R area under curve (AUC) ratio of 1.37 ± 0.32, the stereoselectivity is reversed in poor metabolizers (PM) (S:R AUC ratio of 0.90 ± 0.06].4 Therefore, the same concentrations of the racemate would contain less of the active S isomer and higher concentration of R isomer in poor metabolizers, shifting the ß-blockade effect-concentration relationship to the right. This can lead to loss of cardioselectivity and side-effects associated with b2-blockade.
S-Metoprolol at half the dose of racemate has proved to be effective in the treatment of hypertension. In a randomized, double-blind, double-dummy, comparative clinical trial (n=260) of S-Metoprolol 50 mg ER (Extended Release) with racemic Metoprolol 100 mg ER, the decrease in mean systolic and diastolic blood pressure was comparable in both the groups. However, the responders’ rate (defined as those patients showing a reduction in systolic blood pressure by >20 mm Hg and /or diastolic blood pressure by >10 mm Hg or those achieving a systolic blood pressure reading of <140 mm Hg and/or diastolic blood pressure reading of <90 mm Hg by the treatment) in the S-Metoprolol group was higher by 10.8%, 13.6% (P<0.05) and 7.7% on days 14, 21 and 28 respectively. The absolute improvement of 13.6% on day 21 corresponds to a relative improvement of 23.32% with number needed to treat of only 7.5 (Table 2). The results indicate an earlier response in a large number of patients, and the benefits are obvious.
Table 2. Comparative efficacy of S-Metoprolol 50 mg ER versus racemic Metoprolol 100 mg ER in decreasing the blood pressure (n=260) |
||||
|
S-Metoprolol 50 mg ER (n=128) |
Racemic Metoprolol 100 mg ER (n=132) |
||
Days of treatment |
Systolic BP |
Diastolic BP |
Systolic BP |
Diastolic BP |
Day 0 |
163 ± 13.1 |
100 ± 6.1 |
162.8 ± 11.1 |
100.2 ± 6.8 |
Day 7 |
151± 12.9* |
92.3 ± 7* |
152.7 ± 15.4* |
93 ± 9.6* |
Day 14 |
146 ± 13.4* |
88.8 ± 7.2* |
149.6 ± 14* |
90.4 ± 8* |
Day 21 |
142.5 ± 13.5* |
86.5 ± 6.5* |
144.9 ± 13.6* |
86.9 ± 7.8* |
Day 28 |
138.9 ± 13* |
84.6 ± 6.5* |
141.1 ± 13.8* |
85 ± 6.6* |
Day 35 |
135.6 ± 13.6* |
82.5 ± 6* |
136.9 ± 14.4* |
83.3 ± 6.4* |
Day 42 |
133.2 ± 14.5* |
81.8 ± 6.3* |
132.1 ± 15* |
81.3 ± 6* |
*P<0.0001 as compared to baseline value on day 0 |
||||
In a prospective, post-marketing surveillance study conducted by 133 doctors across India, total of 2000 (M:F=1.99:1) patients of mild to moderate hypertension were studied. This study showed that S-Metoprolol 25/50 mg extended release tablet (Metpure-XL Tablet) was effective, safe and well-tolerated in the treatment of patients with hypertension in clinical practice, including those cases where beta-blockers are used with caution, e.g. COPD, diabetes, dyslipidemia.6
In another open-label, prospective, multicentric clinical study, 104 patients (68 males, 36 females) clinically eligible for beta-blocker therapy, were administered S-metoprolol extended release 50 mg tablets once daily and followed up after 14 and 28 days. This clinical study also confirmed that S-metoprolol extended release tablet was well-tolerated and effectively reduced systolic and diastolic blood pressure (responder rate =90.19%) within 28 days of therapy in patients with hypertension alone or hypertension with concomitant diabetes, obesity, hyperlipidemia, history of dyspnoea and angina.7
In a prospective, open-label, non-comparative clinical study conducted to document the efficacy and tolerability of a fixed-dose combination (FDC) of S-Metoprolol 25 mg and Hydrochlorothiazide 12.5 mg (Metpure-H Tablet) in the treatment of patients (n=50) with mild to moderate hypertension, a significant (P<0.05) reduction in baseline SBP and DBP was seen in 30 days of treatment. There was no worsening of the glycemic or lipidemic status of patients on concomitant anti-diabetic or hypolipidemic therapies. This study showed that FDC of S-Metoprolol 25 mg and Hydrochlorothiazide 12.5 mg was effective and safe in hypertensive patients (including those on anti-diabetic and hypolipidemic therapies).8
SMASH study was another open-label, non-comparative multicentric post-marketing surveillance study conducted in 244 Indian patients suffering from Stage I / Stage II Essential Hypertension who were administered S-Metoprolol extended release tablet in the dosage of 12.5 mg-50 mg per day for a period of 4 weeks. This study showed a statistically significant (P<0.05) reduction in baseline blood pressure and heart rate along with significant improvement in baseline symptom scores of palpitation, dyspnoea, dizziness, weakness and chest pain after S-Metoprolol therapy.9
In an open-label, non-comparative, prospective clinical study, total of 50 hypertensive patients with co-existing COPD with no contraindication for beta blocker therapy were enrolled. Patients received one tablet of S-Metoprolol 50 mg ER once daily for a period of 60 days. Follow-up was done every 15 days during which they were assessed for changes in BP, HR, respiratory symptoms and adverse drug reaction. Spirometry was done before starting therapy and 30 days after therapy. This study showed that the blood pressure reduced significantly (P<0.05) at the same time the mean values of FEV1 and FEV1/FVC did not change significantly on day 30 compared to baseline values. None of the patients reported symptom-based or event-based exacerbation of COPD. This study proved that S-Metoprolol tablet was safe and effective in the treatment of hypertension in patients suffering from COPD.10
An open-label, non-comparative, prospective study in clinical setting was conducted to assess the safety and efficacy of S-Metoprolol succinate extended release tablets in patients with hypertension or angina with coexistent diabetes mellitus. Adult patients of either sex, with hypertension and diabetes mellitus, eligible for monotherapy or combination therapy with S-Metoprolol extended release tablets were enrolled in the study. A total of 55 patients (27 males, 28 females) with type II diabetes mellitus and hypertension completed the study. A total of 43 patients were taking 1/2/3 oral hypoglycemic agents and 16 patients were on insulin. The daily dose of S-Metoprolol ER administered was 50 mg (N=21), 25 mg (N=30), 12.5 mg (N=1) and 100 mg (N=3). Twenty-three patients were on other antihypertensive agents which were continued during therapy with S-Metoprolol. The baseline (before therapy) SBP, DBP and heart rate (HR) reduced significantly on day 45 of therapy. S-Metoprolol as mono-therapy or in combination with other antihypertensive agents was well-tolerated by all the patients.
|
No significant change in baseline F/PP-BSL values was seen on day 45 of therapy. Percentage of patients with PP-BSL more than 140 mg/dL was 87.3 % at baseline and 67.3 % at the end of S-Metoprolol therapy. None of the patients reported hypoglycemic episodes during therapy with S-Metoprolol. This study showed that S-Metoprolol as a mono-therapy or in combination with other antihypertensive agents is effective, safe and well-tolerated in the treatment of hypertensive patients with type II diabetes mellitus.11
In a prospective, comparative study conducted to compare the efficacy and safety of a S-metoprolol ER tablet 50 mg versus a racemate metoprolol ER tablet 100 mg, in the management of angina pectoris, 100 patients with a history of angina pectoris, with or without hypertension, were administered study medications in a sequential 1:1 manner once daily for 8 weeks. The results showed that the reduction in the number of angina attacks from baseline was significant (p< 0.0001) in both the groups with no between-group difference. The response rate in angina (percentage of patients completely relieved of angina attacks clinically) was greater in the S-metoprolol group (72%) when compared to the metoprolol group (62%) (P > 0.05). Both study groups showed significant (p < 0.0001) reduction in baseline systolic blood pressure (SBP), diastolic blood pressure (DBP) and heart rate (HR) in hypertensive patients and a clinically non-significant (p > 0.05) change in normotensive patients. This study proved that in routine clinical practice in the management of angina (with or without coexisting hypertension), S-metoprolol administered at half the dose of the racemate, showed similar efficacy, safety and a trend towards a higher response rate.12
Thus, in view of the known differences (Table 3) between different enantiomers of metoprolol and the efficacy and safety of S-metoprolol, it would be worthwhile to do the chiral switch form racemate metoprolol to S-metoprolol.
Table 3. Differences between Metoprolol enantiomers |
|
S-metoprolol |
R-metoprolol |
b1- selective – blocker |
More selective for b2- blockade |
Cardioselective |
Not-cardioselective |
At high doses does not cause b2 blockade |
Racemate at high doses causes b2 blockade |
Ratio of S:R = 1.37 in extensive metabolisers |
Ratio of R:S = 1.1 in poor metabolisers |
Drug-interactions produce much lesser rise in S enantiomer |
Drug-interactions produce 40-50% rise in R enantiomer |
Allows unopposed stimulation of b2- receptors |
Blocks b2 especially at higher doses. |
References
1. Stoschitzky K, Lindner W, Zernig G. Racemic beta-blockers - fixed combinations of different drugs. Journal of Clinical and Basic Cardiology 1998; 1 (Issue 1): 15-19.
2. Baker JG. The selectivity of ß-adrenoceptor antagonists at the human ß1, ß2 and ß3 adrenoceptors. British Journal of Pharmacology 2005; 144: 317–322.
3. Nathanson JA. Stereospecificity of β adrenergic antagonists: R-enantiomers show increased selectivity for β-2 receptors in ciliary process. J Pharmacol Exp Ther 1988; 245:94-101.
4. Lennard MS, Silas JH, Freestone S, Ramsay LE, Tucker GT, Woods HF. Oxidation phenotype--a major determinant of Metoprolol metabolism and response. N Engl J Med 1982; 307:1558-60.
5. The SMART Trial Study Group. The SMART Trial (S-Metoprolol Assessment in Hypertension Trial). Cardiology Today 2005; IX (4): 222 – 229.
6. SMART-II Study Group. Results of SMART-II study on efficacy and safety of S-Metoprolol extended release tablet. Indian Medical Gazette 2006; CXL(2): 72-75.
7. Aneja P, Srinivas A, Janardhan G. Efficacy and safety of S-Metoprolol extended release tablets in the management of Hypertension – Results of multicentric, prospective, clinical study. Indian Medical Gazette 2005; Vol. CXXXIX(11): 485-487.
8. Singh TSD. Efficacy and Safety of a fixed dose combination of S-Metoprolol 25 mg and Hydrochlorothiazide 12.5 mg Tablet in the Treatment of Mild to Moderate Hypertension. Indian Medical Gazette 2006; Vol. CXL(7):314-317.
9. SMASH Trial Group. S-Metoprolol Assesment in Hypertension (SMASH Trial) Clinical Study of S-Metoprolol Succinate Extended Release Tablet (KIMETXL) in Essential Hypertension. Indian Medical Gazette 2008; Vol CXLII (1): 1-6
10. Mandora VP. Safety and Efficacy of S-Metoprolol Succinate Extended Release tablet in the Treatment of Hypertension Coexisting with COPD – An Open-label, Non-comparative, Prospective Clinical Study. Indian Medical Gazette 2006, CXL(1): 28-32.
11. Talwalkar PG. Safety & Efficacy of S-Metoprolol in the Treatment of Patients with Diabetes Mellitus and Hypertension (SMART-DIMENSION Study). Indian Medical Gazette 2007; CXLI(4): 139-144.
12. Aneja P, Srinivas A, Das Biswas A. Comparative clinical study of the efficacy and safety of a S-metoprolol ER tablet versus a racemate metoprolol ER tablet in patients with chronic stable angina. International Journal of Clinical Pharmacology and Therapeutics 2007; 45(5): 253-258.
13. Reza Mehvar, Dion R. Brocks. Stereospecific Pharmacokinetics and Pharmacodynamics: Cardiovascular Drugs. In: Chirality In Drug Design & Development, Ed.: Indra K. Reddy, Reza Mehvar, Marcel Dekker Inc. USA, 2004; pg 293.
|