ANGIO QUIZ
PCI in Acute Myocardial Infartction: Which Artery to Choose?
Swarnalatha Pallempati, Pramod Kumar Kuchulakanti
Wockhardt Heart Center, Kamineni Hospitals, L B Nagar, Hyderabad, Andhra Pradesh
We describe a 60 year diabetic, normotensive man who presented with acute chest pain. His ECG revealed 2 mm ST elevation in 2, 3 and avf. Patient was in sinus rhythm and hemodynamically stable. He was diagnosed as Acute Inferior wall STEMI and taken up for Primary Angioplasty and Stenting. He was administered Ecospirin 150 mg, Clopidogrel 300 mg and shifted to cath lab. As per our protocol diagnostic coronary angiogram of non-infarcted artery was performed first. To our surprise it revealed normal left main, normal left circumflex artery, but a subtotal occlusion with large thrombus in type III Left Anterior descending artery with TIMI II flow (Figure 1). Subsequent Right coronary artery shoot revealed Right coronary was dominant with distal total occlusion (Figure 2). Thus, sub-total coronary occlusion with a large thrombus large thrombus in LAD was the un-expected finding, with ECG evidence favoring only right coronary artery to be the infarct related artery.
 |
Fig 1 Thrombus in LAD, non-culprit artery |
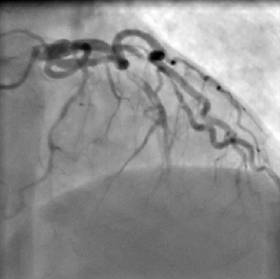 |
Fig 2 Thrombus In LAD with TIMI II flow |
The critical question at this point was which artery to treat?
RCA: ECG changes were present only in inferior leads; LAD: LAD is nearly always the most important artery: Both: Simultaneous plaque rupture is a well known phenomenon; in that case both are culprit arteries and require to be treated.
The second question was that if both require to be treated, which one to tackle first? Since ECG changes were present only in inferior leads a decision was taken to go ahead and do Primary PTCA and Stenting to both RCA followed by LAD. RCA was engaged with AL-1 and the lesion crossed with 0.014” BMW guide wire (Figure 3). Thrombus aspiration was done with Export Catheter (Medtronic Ltd) (Figure 4). While withdrawing the export catheter, the PTCA wire looped and Export catheter had to be removed using gentle force, resulting in a dissection of
 |
| Fig 3 Distal thrombotic occlusion of RCA, culprit artery |
 |
Fig 4 Thrombectomy (Export Catheter) in RCA, note the looping of wire at guide catheter tip |
Correspondence: Dr. swarnalatha Pallempati, consultant Cardiologist, Wockhardt Heart Center, Kamineni Hospitals, L B Nagar, hyderabad, Andhra Pradesh India.
E mail: pkuchulakanti@gmail.com
|
proximal RCA, which was stented with a 3 X 18 mm Bare Metal Stent at 16 atm (Figure 5).
 |
Fig 5 RCA after Angioplasty and Stenting |
Following the RCA angioplasty, LM was engaged with XB 3.5 guide and the lesion in LAD crossed using 0.014” BMW wire and thrombus in LAD extracted with Export catheter (Figure 6). A 3 X 28 mm Titan 2 (Hexacath, India) was deployed at 14 atm with good result (Figure 7).
 |
Fig 6 Export catheter in LAD |
 |
Fig 7 Final Result after Stenting LAD |
Patient remained stable, his cardiac enzymes following angioplasty were: CPK – 765U/L, CPK-MB 74.16 U/L and Trop T 3.91 U/L. 2D Echo revealed normal LV function and no RWMA. He was discharged on day 3 uneventfully.
 |
 |
The Asian Heat Institute and Research Centre situated at Bandra Kurla Complex, Mumbai is a perfect example of what superior standards in cardiac care stand for. Strong infrastructure, dedicated cardiologists and sophisticated technology are just some of the features that the hospital has on offer. Asian Heart Institute requires following Personnel for its expansion. Cardiology- Sr. Consultants, Jr. Consultants, Clinical Associates, Clinical Assistants Cardiovascular Thoracic Surgery - Sr. Consultants, Jr. Consultants, Clinical Associates, Clinical Assistants |
|
|