ENDOVASCULAR STENTING FOR NATIVE COARCTATION IN OLDER CHILDREN AND
ADOLESCENTS USING ADULT SELF –EXPANDING (NITINOL) ILIAC STENTS
Dr.Amar.N.Patnaik, Dr.B.Srinivas, Dr.D.S.Rao
NIZAM’S INSTITUTE OF MEDICAL SCIENCES,PUNJAGUTTA HYDERABAD-500082(AP)
|
|
Introduction
O' Laughlin et al reported the first use of an endovascular stent to treat coarctation of aorta in 1991 (1), which was followed by some clinical reports of successful stent implantation overcoming some of the limitations of balloon angioplasty like residual stenosis, local aortic injury and restenosis. These series have used balloon-expandable stents for relieving coarctation in adults (2, 3, 4, 5, 6, and 7). Later balloon expandable stents had also been tried with encouraging results in older children and adolescents(8,9,10).The balloon expandable stents do not completely appose to the aortic wall and dislodgement or misplacement are not uncommon. Self-expanding nitinol aortic stents adapt better to the wall of the aorta. These stents have recently been reported to be effective in improving results of aortoplasty in aortoarteritis (Takayasu disease) and native coarctation of aorta in adults (11,12,13). We report immediate and short-term follow-up results of self-expandable nitinol (adult) iliac stents implanted in older children and adolescents for native coarctation of aorta.
METHODS AND MATERIAL
Patient population
Thirty two patients(24 males) ,the ages ranging from 6 years to 18 years (mean, 10.2 ± 1.43years) underwent balloon dilation of native coarctation between July2003 and June 2008. Thirty one underwent stent implantation. In one patient 2 stents were used. Patients with age less than 5 years or more than 18 years, those with hypoplastic isthmus, severe co-morbid conditions, associated complex cardiac anomalies and with femoral access problems were excluded.
Procedure
Written informed consent was obtained from the parents of all the patients. Initial evaluation included detailed echocardiographic examination. In 12 cases MRI was done. All patients underwent retrograde femoral artery catheterization under general anesthesia by the Seldinger technique, and 100 units/kg of heparin was administered.
Correspondence: Dr.A.N.Patnaik,24,Anand apartments,7-1-54/2A, D.K.road,Ameerpet, Hyderabad- 500016, AP india
E-mail: anpatnaik@yahoo.com , 040-23743189, 09866229080
|
The coarctation segment was crossed with a 0.035-inch-diameter flexible-tip guide wire, and a pig-tail catheter was passed over the wire into the arch of aorta. Descending thoracic aortography was performed by the 60-degree left anterior oblique view or lateral view to delineate the coarctation segment. Hemodynamic data and angiographic measurement of the coarctation segment, aortic isthmus between the coarctation segment, and the left subclavian artery and the descending thoracic aorta at the level of the diaphragm were measured. A 0.035-inch-diameter, 260-cm-long, extra-stiff guide wire was exchanged. The balloon chosen was with a diameter 2.5 to 3 times that of the narrowest segment but less than 1.5 times the diameter of the aorta proximal to the coarctation. The maximum inflated diameter of the balloon should not exceed the diameter of descending aorta measured at the level of diaphragm.
Bard luminexx vascular stents (Fig.1 A,B) are made up of nitinol; they are self-expandable are loaded onto appropriate sized delivery system. The stents have radio-opaque markers at both ends and are deployed by slow with-drawl of the outer sheath manipulating the trigger on the delivery system after confirming the distal landing point. The size of the stent is chosen is decided based on the target site length and the diameter of the proximal
aortic segment. Prior to the introduction the delivery system was flushed with sterile saline and introduced retrogradely through transfemoral 6F introducer sheath over the extra-stiff guide wire. After deployment, balloon dilation was performed within the stent in all cases by a balloon 2 mm more than the previously used balloon (Fig.2 A,B,C,D). Repeat aortography was performed. Pressure-gradient was recorded across the stented segment. Aspirin (75-150 mg) started the day before and was continued for 6 months after the procedure. Successful procedure is defined as reduction of gradient to less than 20 mmHg or increase in the ratio of the diameter of the coarctation area to the diameter of the descending aorta ( measured at the level of diaphragm) to at least 0.8.
FOLLOW-UP:
Patients were followed up clinically, including complete history, physical examination, and regular assessment of blood pressure in all extremities, antihypertensive medication requirement, and by chest roentgenography. Improvement in hypertension was compared on resting right arm systolic blood pressure recording. Spiral computed tomography (CT) was performed 4 to 6 months after the procedure in 14 patients. Hemodynamic and angiographic restudy was performed in 19 patients after 1 year.
|
 |
Fig-1A. Nitinol made self expanding stent (Bard- luminexx vascular stent). Note the handle with a delivery trigger at the bottom |
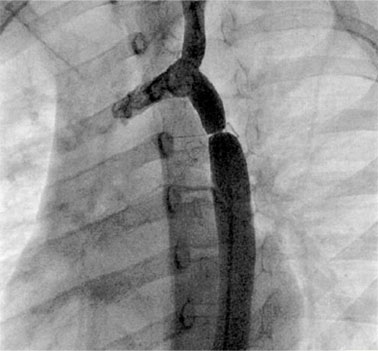 |
Fig-2A. Aortogram showing the discrete native coarctation in 8 year child |
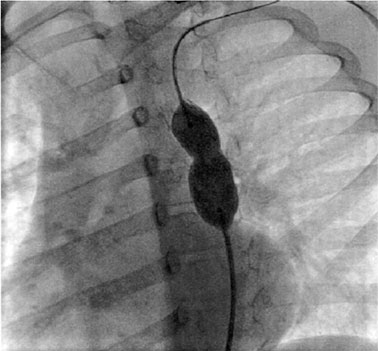 |
Fig-2C.The residual narrowing is dilated with a balloon |
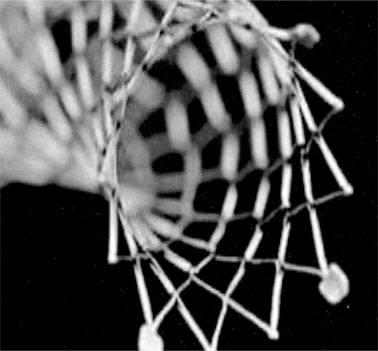 |
Fig-1B. Magnified view of one end of the stent showing the markers |
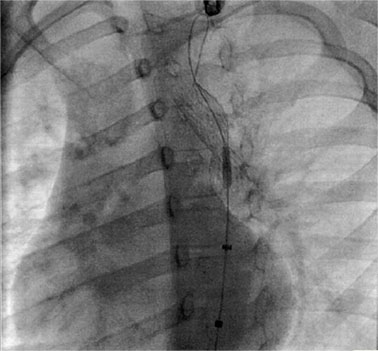 |
Fig.2B. Self-expanding stent deployed across the target lesion |
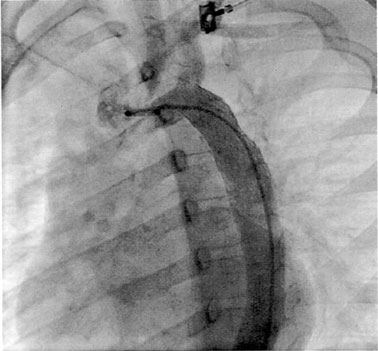 |
Fig-2D. The final result on aortogram |
|
Table-I: Acute results of coarctation stenting
|
|
||||
Pre |
Post |
|
|||
PEAK SYS.GRD |
mmHg (mean-SD) 48.8 ± (23.5) |
2.2 ± (1.86) |
|
||
DIAMETER in mm |
(mean-SD) 5.6± (1.6) |
12.5± (2.6) |
|
||
P-VALUE |
<0.05 |
<0.05 |
|
||
DISCUSSION
Since the early 80s the balloon angioplasty is increasingly used for the treatment of recurrent coarctation and native coarctation. The main limitations of this procedure were aneurysm formation, incomplete relief, and restenosis. Endo-vascular stents were introduced to reduce the recoil and maintain the gain in diameter following the balloon dilatation. Sustained relief of obstruction may decrease the incidence of restenosis. This is particularly important for patients with unfavorable anatomy such as long tubular coarctation and isthmic hypoplasia. Traditionally balloon-expandable stents were used in adults in most studies. There is only a limited experience with the use of stents in children and adolescents. In younger children stents behave as relative stenosis due to the somatic and aortic growth as years pass by.
The self-expanding stents were rarely used in the past. Tyagi et al (12) reported successful use of self-expanding (nitinol) stents producing as good hemodynamic results as with balloon mounted stents and moreover the former showed lesser chance of stent migration. We used self-expandable nitinol stents primarily labelled for use in the iliac arteries for the treatment of native coarctation in children. Such use of self-expanding adult peripheral stents made of nitinol for the treatment of native coarctation in children and adolescents was not reported anywhere before. We used them with an overall success rate of 96.8%. In one patient 2 stents were used because the first stent migrated downwards leaving the lesion partially uncovered. Nitinol stents were easier to deploy and conformed well to aortic walls. Self-expandable nitinol aortic stents are radiopaque ( facilitate more precise positioning) and can be followed up by chest roentgenogram/fluoroscopy. They do not have sharp edges and are atraumatic. The radial strength of nitinol aortic stents is lesser than Palmaz stents. The Palmaz stent, on the other hand, is a rigid, sharp-edged endoprosthesis that may be difficult to deliver in tortuous aorta. It can rupture the delivery balloon, causing vascular injury (14). In the only unsuccessful case in our study, the lesion was 12 mm long, tubular and did not yield even at 16 atm pressure. This case was sent for elective surgery at a later date. There were no deaths or cerebrovascular events. Two cases had femoral artery access related problems (hematoma-1, loss of pulse-1). Twenty five of the 31 successful cases were on regular clinical and
|
|
|
||||||||||||||
|
|
|
||||||||||||||
Re CoA, Recoarctation. * used self-expanding stents |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
||||||||
Pre balloon |
Poststent |
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
Suraz et al, 1999 |
48 |
42/6 |
14 ± 12 (1/2–45) |
42 ± 12 |
3 ± 4 |
1/6 |
2/30 (6%) |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
Hamdan et al, 2001 |
34 |
13/21 |
16 ± 8 (4–36) |
32 ± 12 |
4 ± 11 |
2/4 |
0/4 |
|
|
|||||||
Harrison et al, 2001 |
27 |
20/7 |
30.1 ± 13 (14–63) |
46 ± 20 |
3 ± 5 |
1/0 |
3/18 (17%) |
|
|
|||||||
Ledesma et al, 2001 |
54 |
49/5 |
22 ± 9 (8–49) |
50 ± 20 |
5 ± 8 |
0/6 |
0/1 |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
Tyagi et al* Shah et al Haji et al* Our series* |
21
44
8
32 |
21/0
28/16
6/2
32/0 |
28.6± 11.2 (18–61)
16.9±1.8
15-27
10.2 ± 1.43 |
68.4 ± 22
29.2±1.9
55±15
48.8 ±13.5
|
8.3 ± 4.2
3.7±0.7
5±2
2.2±1.8
|
0/1
1/1
0
0/2 |
0/19
1/44
0
0
|
|
|
|||||||
|
echocardiographic follow-up. On mean follow-up of 1.25 years one had re-coarctation and successful balloon dilation was done. Another case with re-coarctation and persistent hypertension underwent elective surgical repair. In Tyagi’s series one case with self-expanding stent showed significant re-stenosis which could be successfully redilated. (12). Restenosis is an important problem in smaller children (15). Hamdan et al (4) performed repeat dilation in two patients on follow-up. Stent implantation in adolescents and adults is likely to be needed unlike children. Nitinol self-expanding stents, due to their lower radial strength may be more amenable to re-dilatation at a future date. The role of stent redilation in coarctation of aorta is not well studied. Rosenthal in a recent editorial highlighted the present concerns about stent implantation in infants and small children (16). Youngest child in our study was 6 years old.
There were no aortic aneurysms in any case in our study. The formation of aneurysm at the site of stent implantation is a rare late complication with its reported incidence varying from 0 % to 17 % (3-14) (Table-II). Compared to plain balloon aortoplasty stents are believed to minimize local dissections and subsequent aneurysm formation (12). Following surgical repair using synthetic patches the incidence of local aneurysm is reported to occur in 5- 51%. But only a few cases of aneurysms are reported following subclavian flap repair(17,18).
Though stent fracture due to chronic metal fatigue is a possibility on long term follow-up, its occurrence is also very rare. In a recent study(19) of 58 patients(mean age 24±9 years) who underwent balloon angioplasty and followed up to 22 years showed 7% local aneurysm formation and 8% Restenosis.
Limitations
The study involved only a small number and observations need to continue in larger number for drawing firm conclusions. No attempt was done to compare self-expanding stents with balloon expandable stents in this study.
Conclusions
Stent implantation using this readily available low cost adult peripheral self –expanding stents gave gratifying acute and early term results in treatment of coarctation of aorta in older children and adolescents. Ease of deployment, conforming to the aortic anatomy and low cost appears to be the main advantages of these stents. Long term results have to be observed. Improvement in the design and their radial strength, will further improve the results of self-expandable stents.
REFERENCES
1. O’Laughlin MP, Perry SB, Lock JE, Mullins CE. Use of endovascular stents in congenital heart disease. Circulation. 1991; 83: 1923 – 1939.
2 .Dietrich EB, Heuser RR, Cardenas JR, et al. Endovascular techniques in adult aortic coarctation the use of stents for native and recurrent coarctation repair. J Endovasc Surg 1995;2:183-8
3. Suarez de Lezo J, Pan M, Romero M, et al. Immediate and follow-up findings after stent treatment for severe coarctation of aorta. Am J Cardiol 1999;83:400-6.
4. Hamdan MA, Maheshwari S, Fahey JT, et al. Endovascular stents for coarctation of the aortainitial results and intermediate-term follow-up. J Am Coll Cardiol 2001;38:1518-23.
5. Harrison DA, McLaughlin PR, Lazzam C, et al. Endovascular stents in the management of coarctation of the aorta in the adolescent and adult;one-year follow up. Heart 2001;85:561-6.
6. Ledesma M, Alva C, Gomez FD, et al. Results of stenting for aortic coarctation. Am J Cardiol 2001;88:460-2.
7. Cheatham JP. Stenting of coarctation of the aorta. Catheter Cardiovasc Interv 2001;54:112-25.
8.Rao PS. Stents in treatment of aortic coartctation. J Am Coll Cardiol 1997; 30:1853-5
9. Walhout RJ, Lekkerkerker JC,Emst SM et al. Angioplasty for coarctation in different aged patients.Am Heart J 2002; 144:180-6
10.Shah L,Hijazi Z, Sandhu S,Joseph A,Cao QL. Use of endovascular stents for the treatment of coarctation of aorta in children and adults;immediate and midterm results.J Invasive cardiol 2005;17: 614-618.
11Tyagi S, Kaul UA, Arora R. Endovascular stenting for unsuccessful angioplasty of the aorta in aortoarteritis. Cardiovasc Intervent Radiol 1999;22:452-6.
12.Tyagi S, Singh S,Mukhopadhayay S,Kaul UA.Self and balloon expandable stent implantation for severe native coarctation of aorta in adults. .Am Heart J; 146(5):2003
13.Haji-Zeinali AM,Ghasemi M. Coartoplasty with self-expandable stent implantation for the treatment of coarctation of aorta in adults. Arch Iranian Med 2006; 9 (4): 348 – 353
14. Marshall AC, Perry SB, Keane JF, et al. Early results and medium-term follow-up of stent implantation for mild residual or recurrent aortic coarctation. Am Heart J 2000;139:1054-60
15. Duke C, Qureshi SA. Aortic coarctation and recoarctation. To stent or not to stent? J Intervent Cardiol 2001;14:283-96.
16.Rosenthal E. Stent implantation for aortic coarctation; the treatment of choice in adults? J Am Coll Cardiol 2001;38:1524-7.
17.Bell RE,Toyle PR,Aukett M,Young CP,Anderson Dr,Reity JF. Endovascular repair of aneurysms associated with coarctation. Ann Thoracic Surg 2003; 75:530-537
18.Scholz TD,Sato Y,Bolinger L. Aortic aneurysms following subclavain flap repair. Diagnosis on Magnetic resonance imaging. Pediatr Cardiol 2001; 22:153-155
19.Fawzy ME,Fathala A,Osman A,Badr A,Mostafa MA,Gamal M,Bruce D.Twenty –two years of follow-up results of balloon angioplasty for discreet native coarctation of the aorta in adolescents and adults. Am Heart J 2008;156:910-917
|